 This is the story of how I ended up in the hyperbaric chamber at Jacobi Hospital after a terrific dive with some good friends at the Dutch Springs quarry in Pennsylvania. I think that it is a great lesson in how sloppy complacency and the accumulation of several variations from good technique can result in decompression sickness (DCS) - even when diving "conservatively", and without being anywhere near the non-decompression limits. I think that it helps us understand how some divers - like me - actually do deserve those "undeserved" hits. As a surgeon, I know the vital role played by morbidity and mortality conference, where we review all of the possible contributing factors to any bad outcome. Just like in diving, a full analysis of what went wrong goes a long way towards preventing the same problem in the future.
This is the story of how I ended up in the hyperbaric chamber at Jacobi Hospital after a terrific dive with some good friends at the Dutch Springs quarry in Pennsylvania. I think that it is a great lesson in how sloppy complacency and the accumulation of several variations from good technique can result in decompression sickness (DCS) - even when diving "conservatively", and without being anywhere near the non-decompression limits. I think that it helps us understand how some divers - like me - actually do deserve those "undeserved" hits. As a surgeon, I know the vital role played by morbidity and mortality conference, where we review all of the possible contributing factors to any bad outcome. Just like in diving, a full analysis of what went wrong goes a long way towards preventing the same problem in the future.
I am a recreational diver with 532 logged dives at the time of this writing, in October of 2012. I have logged 118 dives in the past year, 203 total in cold water (northeast USA or similar conditions), and 88 at Dutch Springs. On this day I was using my standard cold water equipment - manifolded double 119 tanks, a dry suit with cold water undergarments, and a large camera. The tanks had been topped off from a recent nitrox dive, with a resultant mix of EAN 22. I was diving with a Suunto Vyper air computer, set to the most conservative personal mode. My two buddies were also comfortable with northeast conditions, and we had all been diving together for a few years. The quarry water temperature was 64 degrees at the surface, 55 at depth.
We were delayed by traffic leaving New York City, so in addition to my usual morning cup of coffee, I had another large coffee during the drive. I also had some nuts and an energy bar on the way out, but no other drinks.
We decided to dive in an area of the quarry that we had never visited before - the south shore where there was supposed to be an unmarked airplane wreck in shallow water (20'). We also planned on visiting the pump house on the way out by dropping onto a training platform, following a permanent line, and then following the south shore slope west to look for the plane. Most of my previous dives were in other areas of the quarry, I had been to the pump house once or twice years ago, and never to the south shore. I was leading the dive.
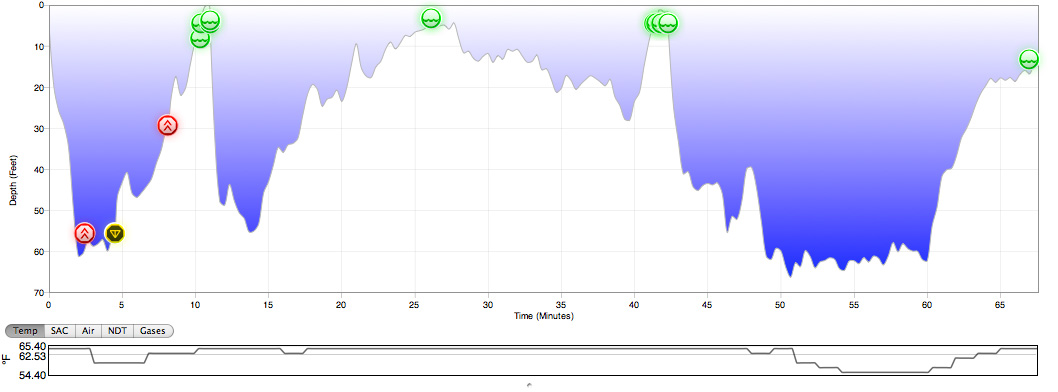
We descended over where we thought the platform was, but did not see it at 25 feet, where all of the other platforms are. Not realizing that this one platform was at 60 feet, I assumed that there was maintenance work being done, or that I was wrong about there being a platform there at all, and swam towards the south wall, abandoning the initial plan to find the pump house first using the line. We followed the slope for a while but I wasn't sure how far we were around the quarry perimeter. I had a rough idea from the surface where the unmarked plane wreck was, so four minutes into the dive I signaled for my buddies to stay put while I would surface to estimate the distance to the area and to determine a compass heading (to possibly cut across the quarry).
I surfaced from 60 feet over 6 minutes and 19 seconds, at an overall rate of 9.5 FPM (well below the typical recommended maximum of 30 FPM). I must have briefly ascended faster than that on two segments of the ascent, since my computer gave me ascent rate violations (ARV) and a "mandatory safety stop", a Suunto penalty for ascent faster than 33 FPM for more than 5 seconds. A review of the raw data dump from my computer showed the peak rates of ascent to be 9.78 feet over one 20 second segment, and 7.48 feet over the second 20 second segment (both still within guidelines), but there may have been even shorter segments where I was moving fast enough to trigger the alert.
Suunto's rationale for the alerts (and mandatory stops) in this situation is that a very brief fast ascent is enough to initiate microbubble formation, which then would make a diver more prone to clinical DCS as the bubbles grow later during "safe" ascents. This proprietary algorithm is claimed to be an advance over the more traditional decompression models that do not account for free gas, just dissolved gas. One downside is that rapidly moving one's arm vertically can cause a wrist mounted computer to give an ARV even if the diver is not ascending that fast, although the five second limit should eliminate most of those false positives.
I waited below the Suunto's 10 foot ceiling depth until the computer cleared the mandatory stop (1 minute), but then surfaced without the standard 3 minute safety stop. On surfacing, I quickly took a bearing and descended back to the team. We proceeded west, ascending slowly as we went until we were in the very shallow water (10-20 feet) around the plane wreck. We stayed in the shallows for approximately 15-20 minutes, then turned back along the shoreline and headed east towards the end of the quarry with the pump house. Realizing that it would be quite a long swim to follow the quarry slope for navigation (one of us was on a single tank), I decided to cut across the east end of the quarry to go to the pump house directly. As we were unfamiliar with this rarely frequented area of the quarry, I decided to surface again for another bearing. I did so at 40 minutes into the dive, from a depth of 28 feet over two minutes (14 FPM), with no ARV, but again with no safety stop. Once I determined the compass heading to the pump house, I descended to the team again, and led them across the quarry to this area. We spent around ten minutes at 60 feet, then did a slow ascent along the shore line and finished the dive with the standard 3 minute safety stop, and about 30 minutes of non-decompression time remaining on my computer.
I felt fine after the dive. We exited the water around 2 PM and headed up to the concession stand for lunch. Around 2:15, I experienced the sudden onset of severe pain in the left upper portion of my abdomen. I sat down and had some soup, which made me feel better. As the abdominal pain resolved, I began to feel tingling in both legs, which progressed to numbness. I stood to walk away from the concession stand, but my legs felt too weak to support me and I sat down on a bench. I asked one of my buddies to go find the medics who are stationed at the quarry, and to bring oxygen. I started breathing oxygen from a non-rebreather mask, and within 15 minutes the symptoms completely resolved. A friend who was a very experienced technical diving and rebreather instructor was also there, and he encouraged me to hydrate aggressively and to take two aspirin.
 I decided not to do another dive, and I also decided to pack the car and head back to New York City. We did so, leaving by around 3 PM; I had one of my buddies drive. On the way back home (a 90 minute drive), I decided to call the Divers Alert Network (DAN) emergency hotline (919-684-9111) and run the situation past them. They strongly encouraged me to get to a hyperbaric chamber, despite the quick resolution of my symptoms. They told me that symptoms can recur after resolution, and that there is the possibility of residual neurological problems. They referred me to Jacobi hospital in the Bronx, which is the only center set up for emergency recompression in the New York City area. I called another friend who is also an instructor and a very experienced diver with knowledge of decompression sickness, and he said the same thing. So my buddies dropped me off at Jacobi, where I was quickly brought into the emergency room without delay (the front desk triage nurse clearly knew the significance of a diving accident). My neurological exam, head CT and chest x-ray were normal, and at around 9 PM I underwent a US Navy Table 6 treatment, breathing 100% oxygen at the ambient pressure of 60 feet, for a PPO2 of 2.7! The treatment lasted approximately five hours; I was accompanied by an RN who had been a navy diver and a commercial diver before going to nursing school to qualify for this job. He monitored me throughout the treatment, especially because of the risk of oxygen induced seizures. I completed the treatment without incident, and was discharged - symptom free - around 2 AM.
I decided not to do another dive, and I also decided to pack the car and head back to New York City. We did so, leaving by around 3 PM; I had one of my buddies drive. On the way back home (a 90 minute drive), I decided to call the Divers Alert Network (DAN) emergency hotline (919-684-9111) and run the situation past them. They strongly encouraged me to get to a hyperbaric chamber, despite the quick resolution of my symptoms. They told me that symptoms can recur after resolution, and that there is the possibility of residual neurological problems. They referred me to Jacobi hospital in the Bronx, which is the only center set up for emergency recompression in the New York City area. I called another friend who is also an instructor and a very experienced diver with knowledge of decompression sickness, and he said the same thing. So my buddies dropped me off at Jacobi, where I was quickly brought into the emergency room without delay (the front desk triage nurse clearly knew the significance of a diving accident). My neurological exam, head CT and chest x-ray were normal, and at around 9 PM I underwent a US Navy Table 6 treatment, breathing 100% oxygen at the ambient pressure of 60 feet, for a PPO2 of 2.7! The treatment lasted approximately five hours; I was accompanied by an RN who had been a navy diver and a commercial diver before going to nursing school to qualify for this job. He monitored me throughout the treatment, especially because of the risk of oxygen induced seizures. I completed the treatment without incident, and was discharged - symptom free - around 2 AM.
In reviewing the events of the day, I have drawn a few conclusions which I hope will make me (and anyone reading this) a safer diver. The biggest take home message is that while most experienced divers take "minor" shortcuts in terms of planning, profiles, and fitness, we usually get away with them, leading to complacency. But physics and physiology are always there in the background. One day, when enough minor things team up to work together, we can put ourselves at real risk of serious injury.
1) A slow, safe ascent should protect us from DCS. But the truth is that every ascent may result in microbubbles - they are simply cleared fast enough by the lungs to prevent their growth and propagation to the point of causing clinical symptoms. A dive with three ascents has more time to allow bubble formation, and to promote their growth. And even ARVs that are so brief as to be below the sampling rate of a dive computer can be enough to start bubble formation. It is still not clear to me whether the ARVs that I received were true or artifact (due to arm motion), but the lesson is clear. Once bubbles are formed, further ascent makes them grow.
2) Good hydration is critical, as dehydration is a well known contributing factor to DCS. Initially, I had assumed that drinking three times as much coffee as usual that morning helped to set me up for the injury, since caffeine acts as a diuretic. After consultation with experts in the field and reviewing the literature, I am less sure that this is the case.
Being well hydrated is important both to prevent injury, and in the early management of DCS symptoms should they occur - this is fairly well established in the medical literature. However, the effect of coffee is less clear, with most recent studies showing that caffeinated beverages are by themselves not a cause of dehydration. The experimental data is consistent with the understanding that while caffeine is a mild diuretic, this effect may be more than offset by the volume of liquid that is consumed. That is, the net fluid change is positive even though part of the water taken in as coffee is lost to urine production. While most dive authorities still suggest hydration (both preventative and for treatment of DCS) with non-caffeinated beverages, the coffee that I drank that morning may not have been a contributing factor to my injury.
3) Good pre-dive planning can prevent the need for unsafe procedures. I had clearly become overly comfortable diving at Dutch Springs, and didn't feel the need to confirm assumptions about an unfamiliar area. I would have never attempted to navigate like this on a dive in the open ocean, but I had become complacent about this location. While we did have a dive plan with two waypoints, once we missed the first platform and had to switch to guesswork, our risks increased. In retrospect, we could have simply relied on the known slope to swim around the edge of the quarry, but I wanted to take more direct routes to the plane wreck and then later back to the pump house, so I took the shortcut of a navigational ascent. Had I determined the depth of the first platform and/or marked down the headings before the dive, I might not have needed to consider that option.
4) While safety stops are not by definition "required", they clearly are one of the things that limits bubble growth and promote outgassing. However, they are frequently omitted in dives with multiple ascents (like an instructor doing a training dive with a group), or in any emergency ascent. I don't know if including them on my two navigation ascents here would have changed the outcome if bubble formation had already started, but it does stand to reason that it might have. In retrospect, this could have helped, but as my buddies were waiting for me below, I was reluctant to add 3 minutes to the 6 minutes that I had already taken for the ascent.
5) Having a high index of suspicion and knowledge of the various symptoms of DCS can make the difference between early successful treatment, and delayed medical attention with residual injury. All divers should familiarize themselves with these symptoms. The numbness and weakness immediately suggested DCS to me, but it was not until afterwards that I realized that abdominal pain can also be a symptom of a spinal cord bubble. Had I not developed the numbness, tingling and weakness in my legs, I might have assumed that the abdominal pain was related to a gastroenterological problem, and not have sought immediate treatment.
6) Oxygen is a vital thing to have on hand in such a situation. Breathing oxygen from a non-rebreather mask (or even better, from a demand regulator if possible) helps accelerate outgassing. I was fortunate to have recognized my injury quickly, and to have had access to emergency oxygen. I assume that all of my own diving will continue to be in a setting where oxygen is available (i.e. Dutch Springs or a professional dive boat). However, if that were ever not to be the case I would consider bringing my own supply.
7) The resolution of symptoms, especially neurological symptoms suggestive of a type II injury, does not necessarily mean that all bubbles have been cleared, or that the symptoms can not recur. In such cases, definitive treatment by recompression is a standard recommendation. What is less clear is evidence that treatment of a diver without symptoms (such as myself) actually changes the eventual outcome. Since it would be ethically impossible to do a study to investigate that (it would require randomizing bent divers to a non-treatment group), it seems that most experts err on the side of caution and recommend recompression treatment even in cases such as mine. I might have been fine had I not opted for treatment in the hyperbaric chamber, but given the relatively low risk of treatment and the concern for a worst-case scenario with residual symptoms, I decided to go ahead with it. This decision was made easier by the fact that I carry DAN insurance. Chamber treatment is very expensive, and many health insurance plans do not cover diving injuries. DAN insurance is inexpensive and worthwhile.
8) Successful treatment of DCS is much more likely the earlier treatment is initiated. I'm happy with the way that things worked out, but had my symptoms persisted at Dutch Springs, it would have been important to get to a nearby chamber as soon as possible. Again, DAN was very helpful with directing me to the nearest center that could provide emergency recompression.
9) Optimizing your breathing mix is a good idea. There are two reasons to use nitrox - either to extend dive time or to increase safety. The trade off is the maximum operating depth (MOD) limitation. Diving an enriched air mixture will add bottom time when compared to air (for a diver whose dives are not limited by tank volume) by extending the non-decompression limits for a given depth. On the other hand, if you breathe nitrox while using air tables (or by setting your computer to air), you will absorb less nitrogen during any given profile compared to air, and thus theoretically make bubble formation and DCS less likely. Some people also claim that nitrox makes them feel better when diving - this is a controversial point without a lot of scientific evidence to support it.
So why was I diving "slightrox" (EAN22) on that day? One of the benefits of having all of your own gear when you dive locally is that you can dive on the spur of the moment, pick trips based on tomorrow's weather forecast, and not worry about running back to a shop to return rental tanks. However, if you keep filled tanks available during dive season, then you may be stuck with a less than optimal mix for any given dive. In general, I keep my tanks filled with EAN28, which will give me extra bottom time, especially on dives close to the MOD. The MOD for EAN28 is 132 feet, so I would not be depth limited on any dive that I am likely to do. Of course, a richer mix would give me even more of an advantage in terms of NDL, but I have been in situations when I unexpectedly got a chance to dive a deeper site with EAN32 in my tanks, and was unable to visit much of the shipwreck. Therefore, EAN28 is a good compromise. On this particular day, I had planned on diving at Dutch Springs when I filled my tanks a few weeks previosly. At the quarry I am rarely limited by NDL, so I chose to save a few dollars and fill my tanks with air. In retrospect, using my regular EAN28 mix might have actually saved me from the consequences of my other errors. In the future, I will not plan on diving right up to the NDL, or I will use nitrox even when it is not needed to extend dive time.
10) Personal risk factors are important, and should be optimized when possible. Some are less easily modified - such as my age (50), the water temperature, and my weight - although I do try to stay in good cardiovascular shape and my dry suit keeps me very comfortable in cold water. We weren't exerting ourselves to any great extent on this dive, but we did cover a lot of distance with some long swims.
One question that remains is whether or not I should be evaluated for a patent foramen ovale (PFO) after DCS. A PFO is a common congential condition (present in up to 35% of people) that in certain circumstances of reversed normal pressure gradients allows blood returning to the heart to mix with blood leaving the heart to the body without passing through the lungs. The contribution of this to DCS is controversial and unclear, although it does make sense anatomically that putting bubbles into the arterial circulation would increase the risk of symptoms. Some studies show a higher incidence of PFO in patients who have had DCS, others find that this association is mainly seen in stroke-like injuries (type IIA) as opposed to milder or transient neurological injuries (type IIB). DAN does not consider a PFO to be a contraindicaion for diving, and notes the limited and mixed evidence on this topic.
11) Recognize and be grateful for your support systems. I am very thankful to DAN and the hyperbaric team at Jacobi, to my friend who helped me initially at the scene of the injury with advice, to Dutch Springs for ensuring that oxygen equipped emergency personnel were available on site, to my other friend who consulted with me on the phone, and of course to both of my dive buddies who not only ran to get me oxygen, water, and aspirin but also gave up a big part of their Saturday night to get me to the Bronx, and even dropped off my dive gear at my apartment!
Dive safe...